Most people assume that fat=stored energy=weight gain. That’s the passive view. The active view is understanding fat as a system – how it forms, where it accumulates, and what it means for long term health.
In the Indian Phenotype Registry, people labelled as just ‘pre-obese’ were already carrying an average of 13% visceral fat. That’s fat hidden deep inside – not visible on the outside but actively driving metabolic dysfunction. And yet, most routine tests miss it. By the time the numbers look worrying, the damage has often begun.
What is visceral fat?
Visceral fat (adipose tissue) is the fat that gets accumulated where it doesn’t belong – around your organs. It gets deposited on your liver, pancreas and intestines; it is metabolically active and harmful. Excess visceral fat leads to systemic inflammation, impairing inulin sensitivity and cellular regulation.
Not all fat is dangerous. When present in healthy amounts, adipose tissues support hormone signalling, energy storage, and thermal regulation. When your fat levels are high – first check for its type, location and volume. Visceral fat, unlike subcutaneous fat, disrupts core metabolic pathways.
Fat and its many roles
Adipose tissue is not a single purpose calorie tank – it is a complex, metabolically active system. It cushions internal organs, insulates the body, and stores energy for future use. It exists in two forms and in two primary locations.
Brown adipose tissue (BAT)
Brown adipose tissue (BAT) is present in much higher quantities in newborns compared to adults, where it is considered nearly absent. BAT generates heat by breaking down fatty acids to produce energy – a process known as non-shivering thermogenesis.
This process is powered by mitochondria. These mitochondria are densely packed in brown fat and rich in iron enzymes – giving the tissue the distinct brown colour. Blood vessels support this process by delivering fuel, and helping to distribute the heat produced.
White adipose tissue (WAT)
White adipose tissue (WAT) plays a small part in heat production. Primarily, it acts as a natural insulator – preventing heat loss and keeping the body warm. WAT’s core function is to store energy in the form of lipids; however it also plays an active role in endocrine signalling, and maintaining insulin sensitivity. Within muscle tissue, WAT provides cushioning, absorbs shock, and reduces friction between muscle layers during movement.
Food provides immediate energy. But when glucose becomes scarce, the body turns to its fat reserves. WAT breaks down stored lipids, releasing fatty acids that fuel organs and sustain energy production. This metabolic flexibility – shifting between glucose and fat, is essential for survival and long term resilience.
White adipose tissues are of two types:
Subcutaneous fat
Subcutaneous adipose tissue (SAT) lies just beneath the skin, and is structurally separate from the body’s internal organs. It acts as a long term energy reserve. Fat stored in the lower body – especially around the hips, thighs, and legs, is linked to better insulin sensitivity and stronger immune regulation compared to fat stored in the upper body. SAT is less inflammatory than other fat types and is considered metabolically protective in moderate amounts.
Visceral fat
Visceral fat is metabolically active, and in excess, releases fatty acids, cytokines, and adipokines directly into the bloodstream. These molecules contribute to systemic inflammation, disrupt lipid metabolism, and impair glucose regulation. Over time, this increases the risk of insulin resistance, type 2 diabetes, cardiovascular disease, and hormone sensitive cancers.
Visceral fat as an endocrine organ
Adipose tissue secretes a range of signalling molecules known as adipokines, including cytokines, hormones, and peptides that influence appetite, metabolism, inflammation, and insulin sensitivity. These molecular messengers form a complex communication network between fat and other systems in the body.
Leptin
Leptin is a satiety hormone released by fat cells after a meal. It signals fullness to the brain, helping regulate appetite and energy balance. Leptin promotes lipid oxidation and kick starts mitochondrial biogenesis – enhancing energy expenditure at the cellular level.
Adiponectin
Adiponectin is a blood based adipokine with anti-inflammatory and insulin sensitising effects. It improves lipid metabolism, reduces insulin resistance, and offers protective benefits against obesity and type 2 diabetes.
Omentin
Omentin is an adipokine produced by visceral fat. It supports insulin sensitivity and may help reduce inflammation. In obesity and insulin resistant states, omentin levels are typically lower – making it a potential marker for metabolic risk. Omentin improves blood vessel function and modulates inflammatory pathways.
Nesfatin
Nesfatin-1 is a peptide hormone expressed in the brain, pancreas, and adipose tissue. It regulates appetite and energy balance but acts through a different mechanism than leptin. It improves both insulin sensitivity and insulin secretion, adding another layer to fat’s role in glucose metabolism.
Resistin
Resistin is secreted by adipose tissue, and is often elevated in obesity. It impairs glucose tolerance, and reduced insulin sensitivity. Animal studies show that resistin contributes to systemic metabolic dysfunction, particularly in the context of chronic inflammation and fat accumulation.
Fat distribution in men and women
Fat distribution and deposition differs by sex and genetics. Women typically carry more body fat than men, storing it in the hips, thighs, and glutes – areas linked to subcutaneous fat. Men tend to accumulate fat around the abdomen, a pattern strongly associated with visceral fat and higher cardiometabolic risk.
Visceral fat accumulation around organs
Visceral fat accumulation increases the risk of metabolic diseases, outweighing the benefits by far. Where fat is stored determines whether it supports function or drives dysfunction.
Liver dysfunction
Excess visceral fat disrupts liver function. Fat deposits release harmful metabolic and endocrine byproducts that enter the liver and impair its role in regulating metabolic processes.
Dyslipidaemia
Dyslipidaemia is the elevated level of lipids, triglycerides, and cholesterol in the blood. It is driven by free fatty acids and inflammatory molecules that interfere with lipid metabolism in the liver, and other tissues.
Inflammation
Excess visceral fat causes inflammation. Fat cells secrete monocyte chemotactic protein-1 (MCP-1), which triggers the infiltration and accumulation of macrophages – a type of white blood cell. Obesity also increases IL-6 levels from visceral fat, further contributing to systemic inflammation.
Insulin resistance
The free fatty acids that are secreted from the dysfunctional adipocites affect muscles and other tissues. The muscles decrease the uptake of glucose. The liver becomes less sensitive to insulin. This affects lipid and glucose metabolism leading to dyslipideamia, and risk for type 2 diabetes. Fat can also accumulate in pancreatic β-cells causing insulin impairment.
How can you measure visceral fat
Weight changes can reflect your goals, but they don’t tell you whether you’re actually burning fat or storing more of it. And that distinction matters, because fat accumulation – especially visceral fat, can silently increase your health risks.
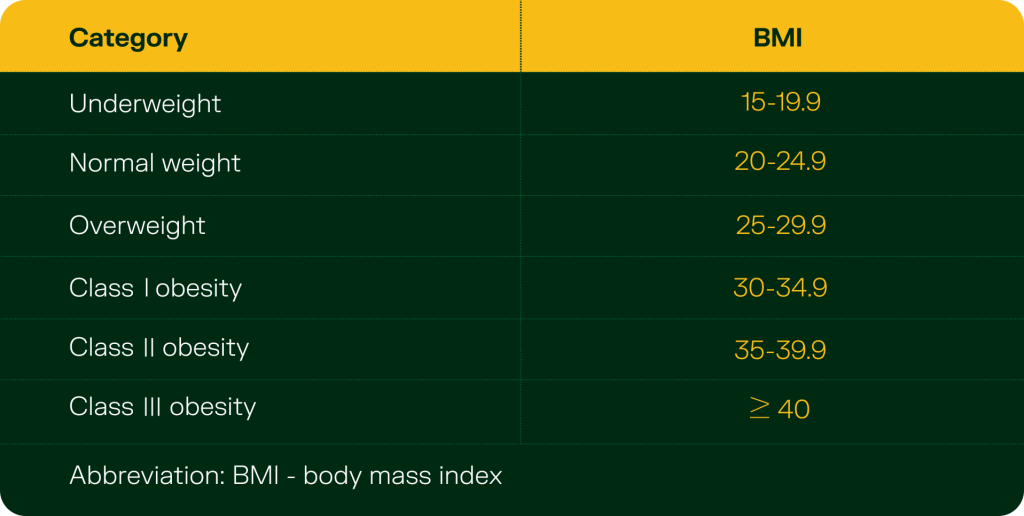
Body mass index (BMI)
Body mass index (BMI) is calculated by dividing weight by height squared (kg/m²) and categorises individuals into general weight ranges. While it provides a rough estimate of total body fat, it fails to distinguish between fat types or locations. BMI does not account for sex, age, or ethnicity, and cannot detect visceral fat specifically.
While both high BMI and visceral fat are often driven by poor diet, low physical activity, and sedentary behaviour, BMI cannot differentiate between harmful fat types. This makes it a limited marker when assessing true metabolic health.
Waist-to-hip ratio
Waist-to-hip ratio is a more accurate indicator of obesity and visceral fat. Use a tape measure to find your waist circumference at its narrowest point, and your hip circumference at its widest. Divide waist by hip. A ratio above 0.90 in men or 0.80 in women is associated with increased metabolic risk.
Dual-Energy X-ray Absorptiometry (DEXA)
DEXA scans are among the most accurate clinical tools for assessing body composition. They use low dose radiation to provide a detailed breakdown of fat distribution – including the relative amounts of subcutaneous and visceral fat. This level of precision enables more targeted and effective intervention.
Gut microbiota and visceral fat accumulation
Visceral fat is not only the result of overeating or inactivity – it’s the result of a deeper biological shift – many of which begin in the gut.
Your gut microbiota digests food, regulates the metabolism, controls inflammation and even influences where fat gets stored. This especially holds true for visceral fat.
Studies show that certain gut bacteria can independently drive visceral fat accumulation, regardless of the diet. Others, like fibre degrading bacteria, can help protect against it. Nutrients like fibre, vitamin E, magnesium, and biotin influence visceral fat, but their effectiveness depends on the microbes in your gut.
In fact, one study found that 69% of fibre’s effect on reducing visceral fat is explained by gut bacteria. Reducing visceral fat more than cutting calories and working out consistently. It’s about restoring the gut ecosystem.
How to reduce visceral fat?
Some gut bacteria can protect against visceral fat build up. Others can worsen it. Many weight loss drugs are out there. But your doctors may not always disclose all the side effects. Functional medicine is all about looking for solutions in the simplest and most basic spaces – lifestyle interventions.
Dietary factors
Diet remains a central focus of research in visceral fat reduction. Low carbohydrate, low fat, keto, high protein, and gluten free diets are all commonly tried – with mixed and highly individualised results. Mediterranean diets, despite being moderately high in fat, show better result in reducing visceral fat. This is most likely due to its richness in unsaturated fats, polyphenols, and fibre, which nourish beneficial gut bacteria.
Other approaches include:
- Anti-inflammatory diet: cruciferous vegetables, foods rich in polyphenols, omega-3
- Microbiome-supportive foods: prebiotic fibers, resistant starches
- Removal of visceral-fat drivers: refined carbs, trans fats, seed oils, ultra-processed foods
- Possible therapeutic fasting windows: Circadian-based eating
Physical activity
Aerobic workouts and high intensity training yield the strongest results. Aim for at least 150 minutes of moderate intensity exercise each week.
Extended periods of movement, especially during or after fasting, deplete the body’s primary energy stores like glucose and glycogen. This forces the body to turn to fat reserves, including visceral fat, for fuel.
The most effective strategy is a combination of nutrient dense eating and regular physical activity. Together, they improve body composition, lower inflammation, and support a healthier gut microbiome. Even if the number on the scale doesn’t change, these habits can significantly reduce visceral fat and improve long term health outcomes. You create the conditions for visceral fat to reduce naturally and sustainably.
This isn’t just about looking lean. It’s about protecting your organs, balancing your metabolism, and extending your health span.